Time-to-First-Patient (FPI): The Most Expensive Phase of a Clinical Trial

Time-to-first-patient is the most expensive phase of a clinical trial. It is the stretch of time between the moment a study is ready to begin and the moment its first participant receives the first dose. The industry shorthand for this milestone is FPI, short for first patient in. For sponsors, it is the single hardest part of a trial to control, and the easiest to underestimate.
During this window, the trial is fully funded but not yet generating evidence. Regulatory work is done. Contracts with research sites are signed. The study drug has been manufactured. Operational teams are paid. Every day spent waiting for the first participant is a day of full spend with nothing to show for it.
Sponsors often do not realize how slowly first patient in is approaching until the slip is already weeks deep. The reasons are predictable, but they are rarely visible from the inside.
What time-to-first-patient really is
Time-to-first-patient measures the length of time between when a clinical trial is operationally ready and when its first participant is dosed. The clock typically starts at study activation or site activation, depending on the sponsor's preferred milestone. The clock stops when the first participant takes the first dose of the study drug. Some sponsors track a related metric called FPFV, or first patient first visit, but it points to the same underlying concern. How long does it take to move from being ready to begin to actually having begun?
This phase of a trial is unusually expensive. By the time a study is operationally ready, the sponsor has already paid for protocol design, regulatory submissions, site contracts, vendor agreements, drug supply, and operations staffing. The investment is fully in motion. What is missing is the one thing that justifies all of it: enrolled participants generating clinical data. Until a participant is dosed, the trial earns nothing for the money already committed.
Slow time-to-first-patient also has consequences beyond cost. It pushes back every subsequent milestone in the trial, including database lock, statistical analysis, regulatory submission, and ultimately approval. The hidden cost of slow recruitment is felt across the entire timeline, and in therapeutic areas with high unmet need, those delays matter even more.
Why time-to-first-patient drags
The reasons time-to-first-patient runs slow are not usually about effort. Sponsors, sites, and recruitment teams typically work hard. The issue is the order in which the work happens.
In most trials, candidate identification only begins after a research site has been activated. That means recruitment starts from zero at the exact moment the study is most expensive to operate. Sites need time to identify potential participants in their patient population, schedule screening visits, and check eligibility against the protocol. Even when sites move quickly, they are starting from a standing position.
A second issue is that many candidates who reach the screening visit are not actually eligible. They look eligible on the surface, but a closer review of their medical history, current medications, or other criteria reveals a mismatch. By the time the mismatch is discovered, the site has spent hours on the visit and the participant has spent goodwill on a process that did not lead anywhere. This is known as a screen failure, and across the industry it is one of the largest drains on early enrollment momentum.
A third issue is that sponsors usually cannot see, in real time, how each site is performing in the recruitment phase. Enrollment reports come in on monthly or quarterly cycles. By the time a slow site is flagged, weeks of trial timeline have already been lost. There is rarely an early warning system that catches a recruitment problem before it shows up in the enrollment numbers. The ongoing challenge of clinical trial recruitment is, in many ways, this exact gap between what is happening on the ground and what sponsors can see in time to act on it.
How DecenTrialz solves the time-to-first-patient problem
DecenTrialz is a clinical trial recruitment and pre-screening platform built specifically to fix the problems behind slow time-to-first-patient. The platform addresses the recruitment funnel at every point where time is normally lost.
DecenTrialz begins by using AI-powered participant matching to identify potential participants against a study's eligibility criteria. This matching can begin during the regulatory and contracting phase of a trial, before research sites are fully activated. By the time sites open their doors, a candidate pipeline is already in place. The recruitment funnel no longer starts from zero on the day of site activation. It starts from a population of participants who have already been identified as likely matches for the protocol.
Once candidates are identified, a registered nurse on the DecenTrialz team conducts an initial pre-screening review of each one. This review filters out candidates who would not pass the formal screening visit at the research site. By catching mismatches before participants ever travel to a site, DecenTrialz reduces the screen failure rate that traditionally slows down early enrollment. The candidates who do reach the site are far more likely to move through screening successfully and enroll in the study.
After pre-screening review, DecenTrialz makes a structured referral to the authorized research site for the trial. Final eligibility determination, informed consent, and enrollment remain with the study team at the research site, where they should be. DecenTrialz handles the front of the recruitment funnel; the site handles the clinical decisions that only the study team can make. This streamlined participant intake workflow is what turns a traditionally slow handoff into a smooth, fast-moving sequence.
Throughout the process, sponsors see what is happening in real time. From the first day of recruitment, the DecenTrialz dashboard shows how many candidates have been identified, how many have cleared nurse pre-screening, how many have been referred to sites, and how many have been enrolled and dosed.
What sponsors gain from getting to first patient faster
When time-to-first-patient is shortened, every milestone downstream moves up with it. The study reaches database lock sooner. Statistical analysis begins sooner. Regulatory submission happens sooner. And the eventual therapy reaches the patients who need it sooner.
Beyond the timeline, sponsors also gain operational confidence. Data-driven recruitment dashboards mean that problems in the recruitment funnel can be identified and addressed early. If a site is not producing the expected flow of referrals, the sponsor sees it within days, not months. Adjustments can be made while there is still time to recover. The recruitment phase, traditionally the most opaque part of trial operations, becomes one of the most transparent.
For clinical operations teams, the shift is from waiting and hoping to seeing and acting. Each step in the funnel is visible, measurable, and connected to the next. The trial does not have to begin with a slow ramp. It can begin with momentum.
A faster path to first patient
The most expensive phase of a clinical trial does not have to be the slowest. With the right recruitment infrastructure in place before the first site is activated, sponsors can move from ready to begin to actually beginning in far less time than the traditional model allows.
DecenTrialz exists to make that possible. By combining AI-assisted participant matching, nurse-led pre-screening review, structured referral to authorized research sites, and real-time recruitment dashboards for sponsors, DecenTrialz brings the recruitment funnel forward in the trial timeline, removes the mismatches that slow enrollment, and gives sponsors a clear view of progress from day one. The result is a trial that gets to its first dose sooner, and to its conclusion sooner.
Was this article helpful?
Similar Blogs
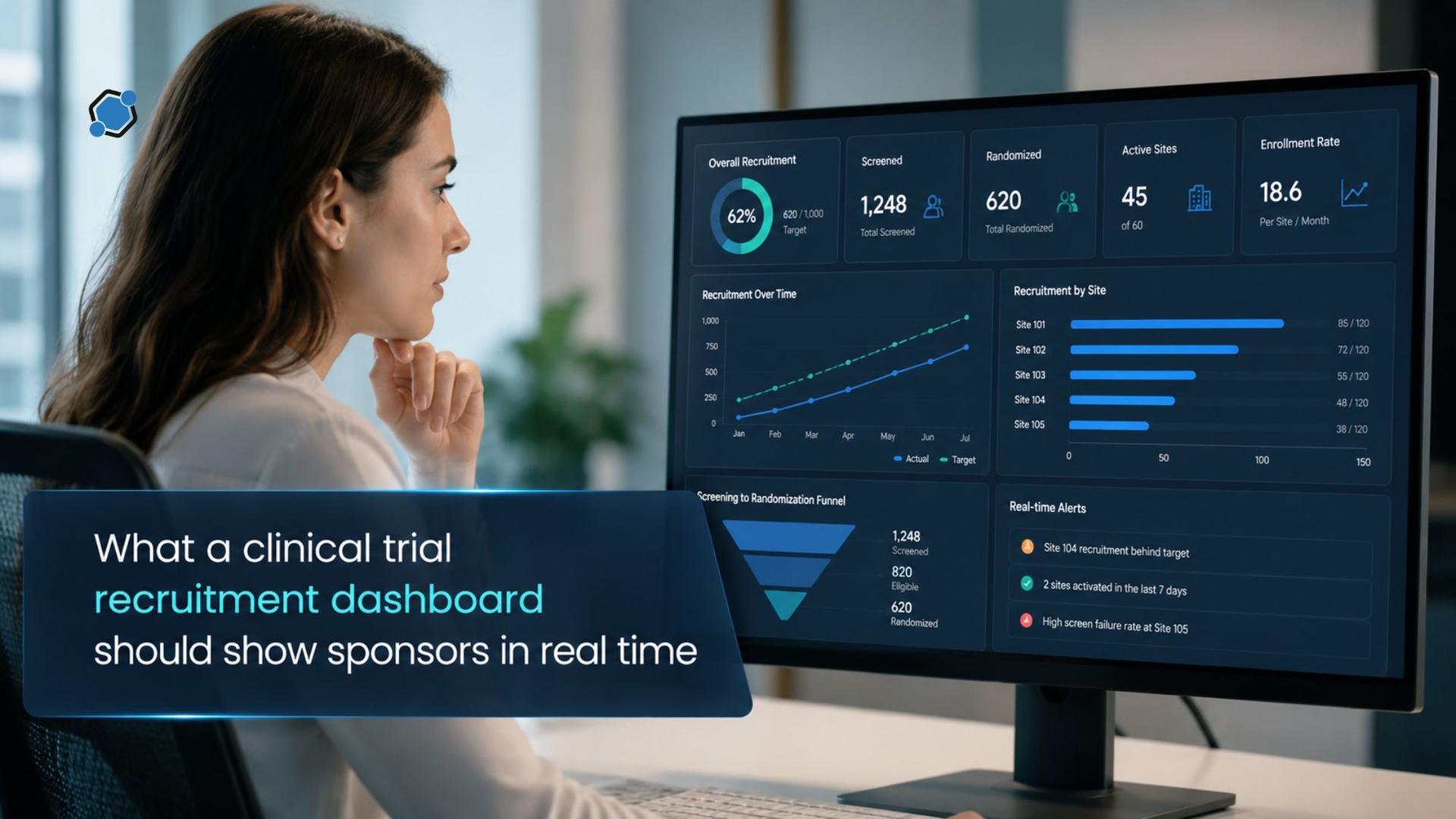
What a clinical trial recruitment dashboard should show sponsors in real time
Adding a site in month three of a twelve-month enrollment period is a routine operational ...

Choosing the right patient recruitment partner for your clinical trial
Few decisions shape a clinical trial as directly as the choice of a patient recruitment pa...

How sponsors build a diverse enrollment pipeline without slowing the study
Diverse enrollment and fast enrollment tend to get talked about as if they were pulling ag...
Stay Informed. Stay Connected.
Get updates on verified clinical trials, emerging treatments, and research breakthroughs directly in your inbox. No spam, just science that matters.
