Breakthrough Therapy Designation: The FDA Program That Helps Promising Drugs Reach Patients Sooner

In 2012, the U.S. government gave the Food and Drug Administration a new tool for handling drugs that look unusually promising. The program was named with care: not “fast-track,” not “priority review,” but breakthrough therapy designation. Every word was meant to carry weight.
Fourteen years later, the word that has carried the most weight is the one in the middle. Breakthrough. To a drug company, it is a regulatory status with specific criteria. To everyone else, it sounds like a promise. The gap between those two readings is where most of the confusion about the program lives.
This article walks through what the designation is, what it changes during development, and what it ends up meaning in practice.
What “breakthrough” means inside the FDA
The designation has a narrow definition. A drug qualifies only if it is being developed for a serious or life-threatening illness, and only if early clinical data suggests it may offer a substantial improvement over the treatments already available.
“Substantial improvement” is the part that does the screening. There is no fixed numerical threshold, because the answer depends on what the disease is and what the existing options are. A 15 percent gain in survival is substantial for a cancer with no good treatments. The same number, for a condition that already has effective therapy, is not.
The bar is high on purpose. Less than 40 percent of requests for the designation are granted. The rest are denied, often because the early evidence is interesting but does not yet show a clear leap over current care.
A useful parallel is the Orphan Drug Act of 1983, an earlier federal mechanism aimed at a different unmet need: drugs for rare diseases whose patient populations are too small to justify the usual commercial investment. The two programs work on different principles, but they share a premise. When the science and the patient need both point in the same direction, the regulator has tools to help the path forward. Our blog The 1983 Law That Changed Rare Disease Research, and What It Means for Patients Today covers that earlier program.
What the designation actually changes during development
By the time a drug becomes eligible for the designation, it has already been through years of laboratory research and the early stages of human testing. Our blog Phase 0 Clinical Trials: What They Are and Why They Exist explains the earliest checkpoint in that process. The designation typically arrives around the middle of development, when there is enough early clinical data for the FDA to evaluate but enough late-stage work still ahead for the program’s benefits to make a real difference.
A drug that receives the designation does not skip steps. Every trial still has to be run. Every safety question still has to be answered. What changes is the level of FDA involvement, and the speed at which paperwork moves between the agency and the drug company.
Three changes are concrete. First, senior FDA staff are assigned to the drug’s development and meet with the company often. This is not a courtesy. It is the program’s most important feature. Decisions that would normally sit for weeks get made in days. Trial designs are tightened before they are launched. Studies that would have produced redundant data are dropped before money is spent on them.
Second, the agency allows what is called rolling review. Most drug applications are submitted all at once, after every study is complete. With rolling review, completed sections can be submitted as they are ready, and the FDA begins reviewing them immediately. This compresses the gap between the end of testing and a final decision.
Third, the drug becomes eligible for every other expedited program the agency offers, including priority review, which shortens the FDA’s final decision window from ten months to six.
The combined effect, over the past decade, has been measurable. Drugs with the designation reach approval meaningfully faster than comparable drugs without it, without an observable increase in safety problems afterward. Independent research has put the time savings in the range of one to two years for late-stage development. Our blog How Clinical Trials Advance Medicine and Change Lives covers the broader trial process every drug has to move through, regardless of designation.
Many trials of breakthrough-designated drugs are recruiting participants right now. A search at decentrialz.com returns active studies for a given condition.
Where the designation ends up mattering, and where it doesn’t
Some of the most consequential drugs of the past decade carried the designation during their development. Keytruda, the cancer immunotherapy now used across more than twenty different cancer types, received it. Sofosbuvir, the hepatitis C drug that turned a chronic, often fatal infection into a curable one, received it. Casgevy, the first gene-editing therapy approved in the United States, received it.
These are not minor footnotes in medicine. They are some of the most significant therapeutic advances of the modern era, and the designation was part of how they reached patients on the timelines they did.
The designation, however, is not what made them work. The science did. The designation made the process around the science more efficient. A drug that ultimately fails its late-stage trials will still fail them with the designation in hand. A drug that works will work either way, but it may reach patients meaningfully sooner with the designation than without.
This distinction matters because the word “breakthrough” suggests a verdict on the drug itself. It is not. It is a verdict on the early evidence. Some designated drugs go on to fail their late-stage trials. Many never reach approval at all.
A useful way to read the designation is as a signal that a drug is being taken seriously by both its developer and the regulator, not as a guarantee about what it will eventually deliver. Our blog Gene Editing Has Reached Real Patients. Here’s What CRISPR Clinical Trials Look Like Now covers one specific case where the science delivered. Our blog From COVID-19 to Cancer: How mRNA Technology Is Transforming Modern Medicine covers a broader platform where the designation is currently being applied to multiple drugs in development, with outcomes still to be determined.
DecenTrialz is a platform that connects people to clinical trials they may be eligible for. You provide basic information about your condition and history, get matched with studies that fit, and speak with a nurse who pre-screens you and explains what each study involves before you decide. The research team running each study makes the final eligibility and enrollment decisions. Start a search at decentrialz.com.
Was this article helpful?

Similar Blogs

Master protocols and portfolio strategy: choosing between basket, umbrella, and platform designs
The default way to develop a drug used to be one trial per question. One asset, one indica...
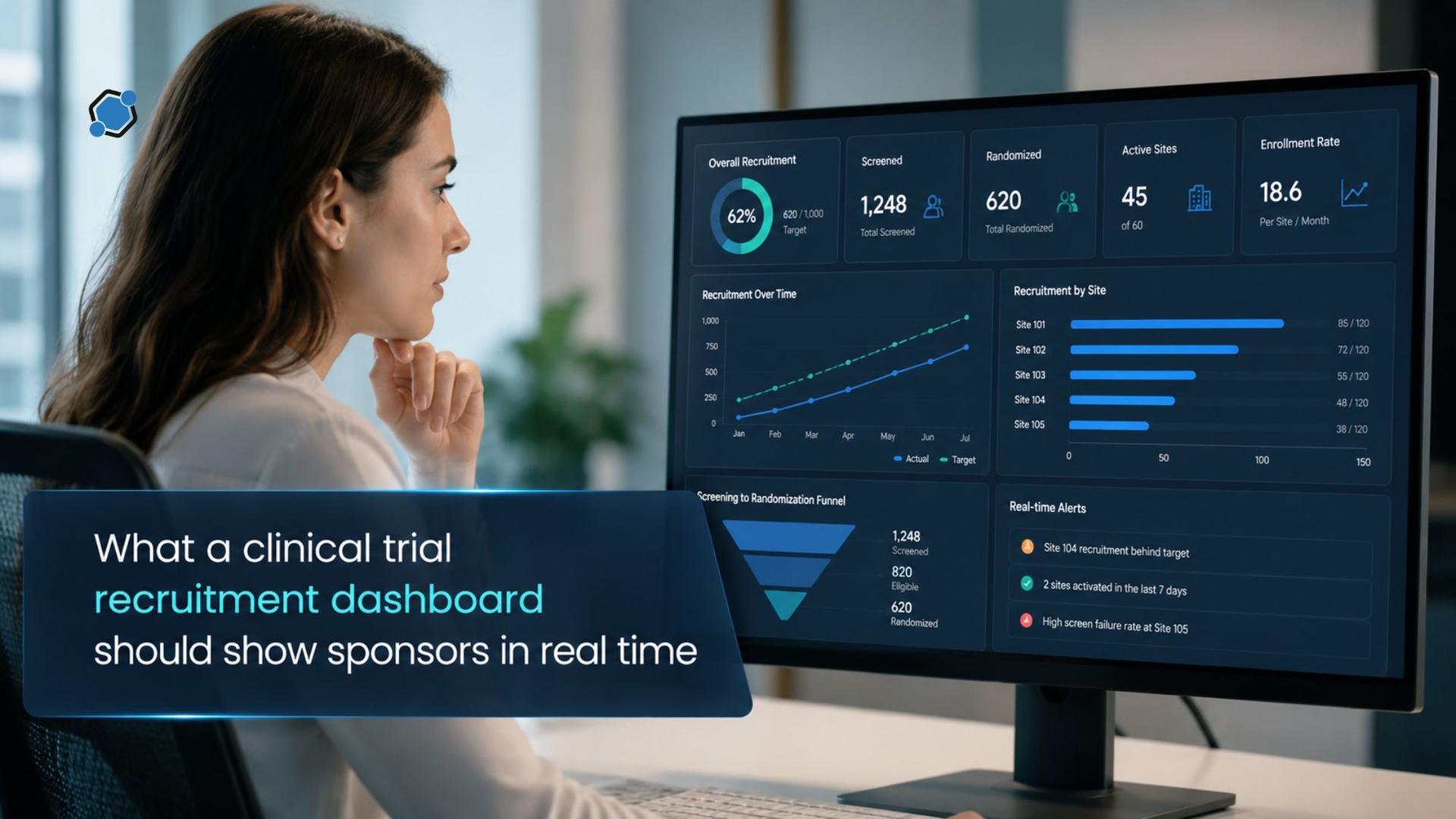
What a clinical trial recruitment dashboard should show sponsors in real time
Adding a site in month three of a twelve-month enrollment period is a routine operational ...

Choosing the right patient recruitment partner for your clinical trial
Few decisions shape a clinical trial as directly as the choice of a patient recruitment pa...
Stay Informed. Stay Connected.
Get updates on verified clinical trials, emerging treatments, and research breakthroughs directly in your inbox. No spam, just science that matters.
